*Defined as health-related quality of life and functional capacity.1
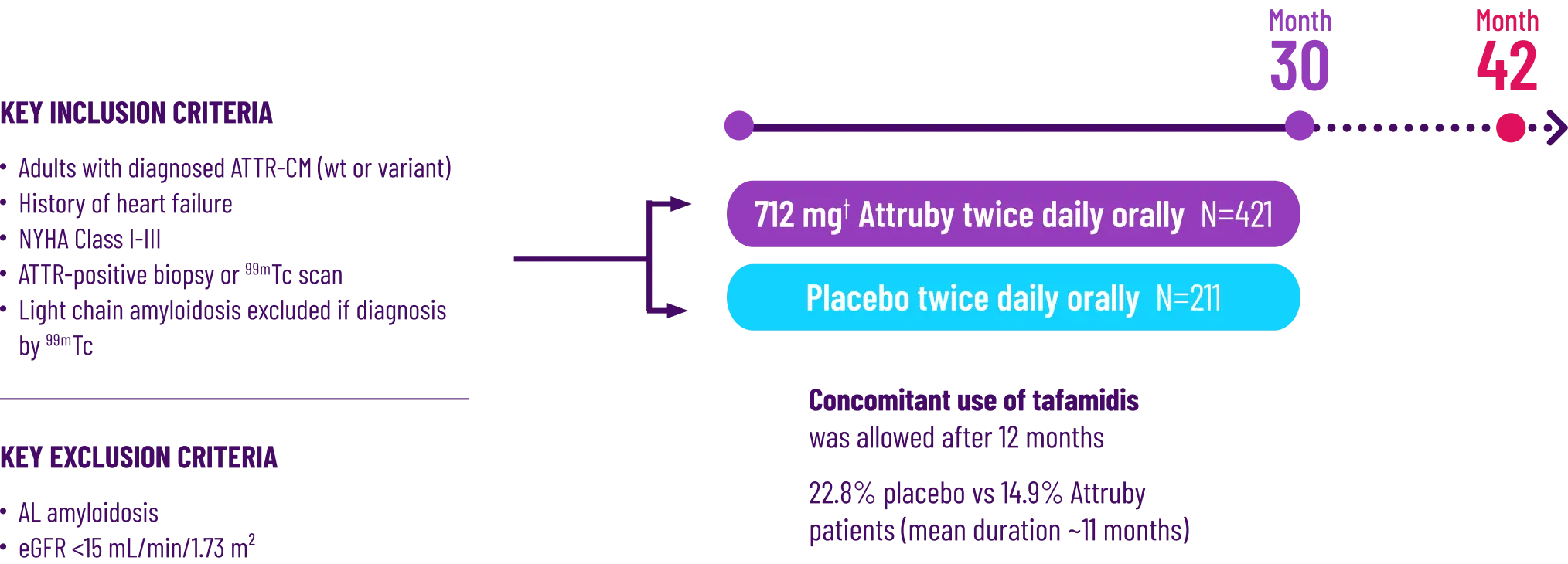
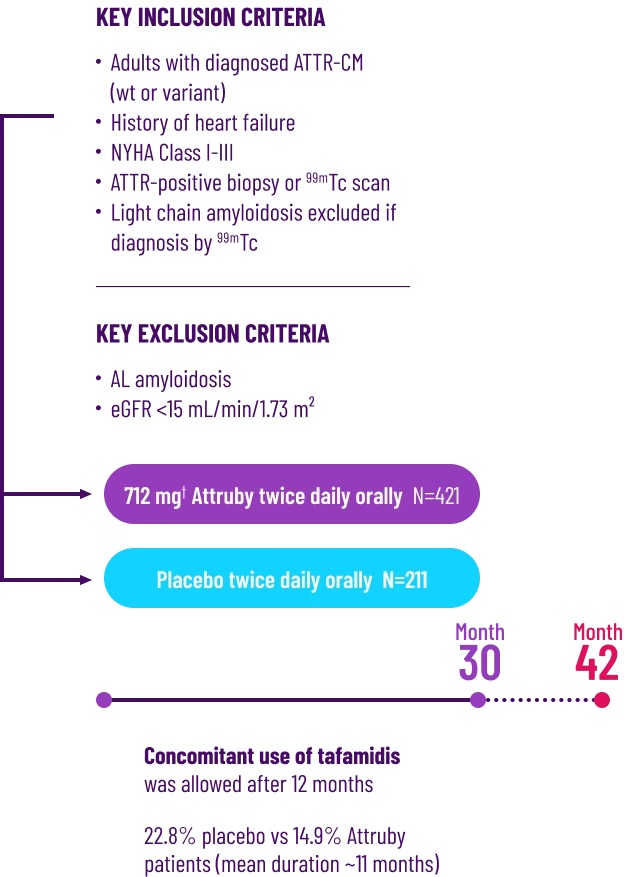
†Attruby 712 mg twice daily is equivalent to Attruby HCl 800 mg twice daily.3
‡Analysis conducted using the stratified F-S test .1
.1
§These secondary endpoints are prespecified and non-alpha protected.3,6
||Based on ITT population of 632 patients, including 21 who had stage 4 CKD. The ITT population was defined as all randomized participants who received at least
1 dose of study drug and had at least 1 postbaseline efficacy evaluation and included participants who had a baseline eGFR <30 mL/min/1.73 m2.2
¶i.e., NYHA Class I and II.3
#IXRS stratification factors.2
6MWD=6-minute walk distance; 99mTc=technetium labeled pyrophosphate (PYP) or bisphosphonate (eg, DPD); ACM=all-cause mortality; AL amyloidosis=light chain amyloidosis; ATTR=transthyretin amyloidosis; ATTR-CM=transthyretin amyloid cardiomyopathy; ATTRv=variant transthyretin-mediated amyloidosis; ATTRwt=transthyretin amyloidosis wild-type; CFB=change from baseline; CKD=chronic kidney disease; CV=cardiovascular; CVH=cardiovascular-related hospitalization; CVM=cardiovascular-related mortality; eGFR=estimated glomerular filtration rate; F-S test=Finkelstein-Schoenfeld test; ITT=intent-to-treat; IXRS=Interactive Web Response Systems; KCCQ-OS=Kansas City Cardiomyopathy Questionnaire Overall Summary; mITT=modified intent-to-treat; NT-proBNP=N-terminal pro–B-type natriuretic peptide; NYHA=New York Heart Association; TTR=transthyretin; WT=wild-type.
References: 1. Attruby. Prescribing information. BridgeBio Pharma, Inc.; 2024.
2. Gillmore JD, Judge DP, Cappelli F, et al. Efficacy and safety of acoramidis in transthyretin amyloid cardiomyopathy. N Engl J Med. 2024;390(2):132-142. doi:10.1056/NEJMoa2305434
3. Data on file. BridgeBio, Inc.; 2024-2025.
4. Ioannou A, Patel RK, Razvi Y, et al. Impact of earlier diagnosis in cardiac ATTR amyloidosis over the course of 20 years. Circulation. 2022;146(22):1657-1670. doi:10.1161/
CIRCULATIONAHA. 122.060852
5. Gillmore JD, Judge DP, Cappelli F, et al. Efficacy and safety of acoramidis in transthyretin amyloid cardiomyopathy [study protocol]. N Engl J Med. 2024;390(2): 132-142. doi:10.1056/NEJMoa2305434
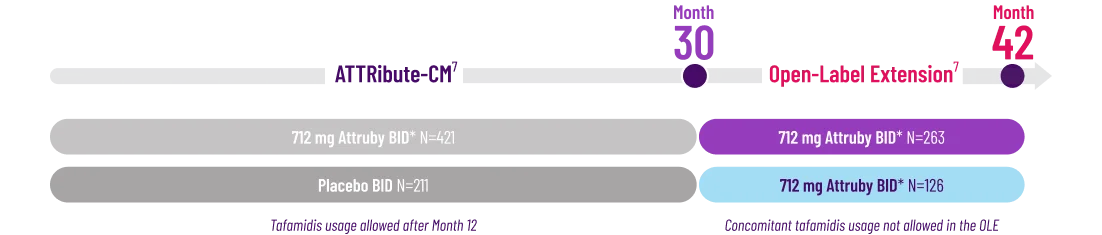
6. Judge DP, Gillmore JD, Alexander KM, et al. Long-term efficacy and safety of acoramidis in ATTR-CM: initial report from the open-label extension of the ATTRibute-CM trial. Circulation. 2025;151(9):601-611. doi:10.1161/CIRCULATIONAHA.124.072771
7. Judge DP, Gillmore JD, Alexander KM, et al. Long-term efficacy and safety of acoramidis in ATTR-CM: initial report from the open-label extension of the ATTRibute-CM trial. Circulation. 2025;151(9)(suppl 1):1-4. doi:10.1161/CIRCULATIONAHA.124.072771