Attruby delivers near-complete in vitro TTR stabilization6,9
Attruby is the only FDA-approved treatment described as achieving near-complete (>90%) in vitro TTR stabilization in its label — no other product label includes this distinction.
References: 1. Liz MA, Coelho T, Bellotti V, Fernandez-Arias MI, Mallaina P, Obici L. A narrative review of the role of transthyretin in health and disease. Neurol Ther. 2020;9(2):395-402. doi:10.1007/s40120-020-00217-0
2. Vieira M, Saraiva MJ. Transthyretin: a multifaceted protein. Biomol Concepts. 2014;5(1):45-54. doi:10.1515/bmc-2013-0038
3. Ruberg FL, Grogan M, Hanna M, Kelly JW, Maurer MS. Transthyretin amyloid cardiomyopathy: JACC state-of-the-art review. J Am Coll Cardiol. 2019;73(22):2872-2891. doi:10.1016/j.jacc.2019.04.003
4. Kittleson MM, Maurer MS, Ambardekar AV, et al. Cardiac amyloidosis: evolving diagnosis and management: a scientific statement from the American Heart Association. Circulation. 2020;142(1):e7-e22. doi:10.1161/CIR.0000000000000792
5. Witteles RM, Bokhari S, Damy T, et al. Screening for transthyretin amyloid cardiomyopathy in everyday practice. JACC Heart Fail. 2019;7(8):709-716. doi:10.1016/j.jchf.2019.04.010
6. Attruby. Prescribing information. BridgeBio Pharma, Inc.; 2024.
7. Gillmore JD, Judge DP, Cappelli F, et al. Efficacy and safety of acoramidis in transthyretin amyloid cardiomyopathy. N Engl J Med. 2024;390(2)(Suppl 1):1-34. doi:10.1056/NEJMoa2305434
8. Gertz MA, Benson MD, Dyck PJ, et al. Diagnosis, prognosis, and therapy of transthyretin amyloidosis. J Am Coll Cardiol. 2015;66(21):2451-2466. doi:10.1016/j.jacc.2015.09.075
9. Gillmore JD, Judge DP, Cappelli F, et al. Efficacy and safety of acoramidis in transthyretin amyloid cardiomyopathy. N Engl J Med. 2024;390(2):132-142. doi:10.1056/NEJMoa2305434
10. Hammarström P, Jiang X, Hurshman AR, Powers ET, Kelly JW. Sequence-dependent denaturation energetics: a major determinant in amyloid disease diversity. Proc Natl Acad Sci USA. 2002;99(suppl 4):16427-16432. doi:10.1073/pnas.202495199
11. Almeida ZL, Vaz DC, Brito RMM. Transthyretin mutagenesis: impact on amyloidogenesis and disease. Crit Rev Clin Lab Sci. 2024;61(7):616-640. doi:10.1080/10408363.2024.2350379
12. Hornstrup LS, Frikke-Schmidt R, Nordestgaard BG, Tybjaerg-Hansen A. Genetic stabilization of transthyretin, cerebrovascular disease, and life expectancy. Arterioscler Thromb Vasc Biol. 2013;33(6):1441-1447. doi:10.1161/ATVBAHA.113.301273
13. Judge DP, Heitner SB, Falk RH, et al. Transthyretin stabilization by AG10 in symptomatic transthyretin amyloid cardiomyopathy. J Am Coll Cardiol. 2019;74(3):285-295. doi:10.1016/j.jacc.2019.03.012
14. Maurer MS, Judge DP, Gillmore JD, et al. Early increase in serum transthyretin by acoramidis independently predicts improved survival in TTR amyloid cardiomyopathy. J Am Coll Cardiol. 2025;85(20):1911-1923. doi:10.1016/j.jacc.2025.03.542
15. Sarswat N, Ambardekar A, Taubel J, et al. Acoramidis-mediated early increase in serum transthyretin is associated with lower cardiovascular-related hospitalizations and mortality: insights from the ATTRibute-CM study. Poster presented at: American College of Cardiology Annual Scientific Meeting; March 29-31, 2025; Chicago, IL.
16. Data on file. BridgeBio, Inc.; 2024-2025.
T119M is a naturally occurring stabilizing variant of TTR
In TTR VARIANT CARRIERS11
The V30M mutation can induce structural alterations that lead to amyloid deposition. Researchers found that the T119M mutation may mitigate the pathogenic effects of the V30M mutation
Carriers of T119M had higher levels of serum TTR due to slower clearance of the protein from serum, as assessed by clearance studies
TTR is a key transport protein that binds to and transports
vitamin A and thyroxine throughout the body, and it performs
its function when it's present and stable.1,2
In ATTR-CM, aging or genetic variants can cause TTR to
destabilize and break apart into monomers, which misfold and
accumulate as toxic amyloid fibrils throughout the body,
including in the myocardium.3-5
By preserving TTR structure and slowing toxic amyloid fibril formation,
TTR stabilizers may help alter the natural course of the disease.8
It's a marker you can measure. And data you can stand behind.
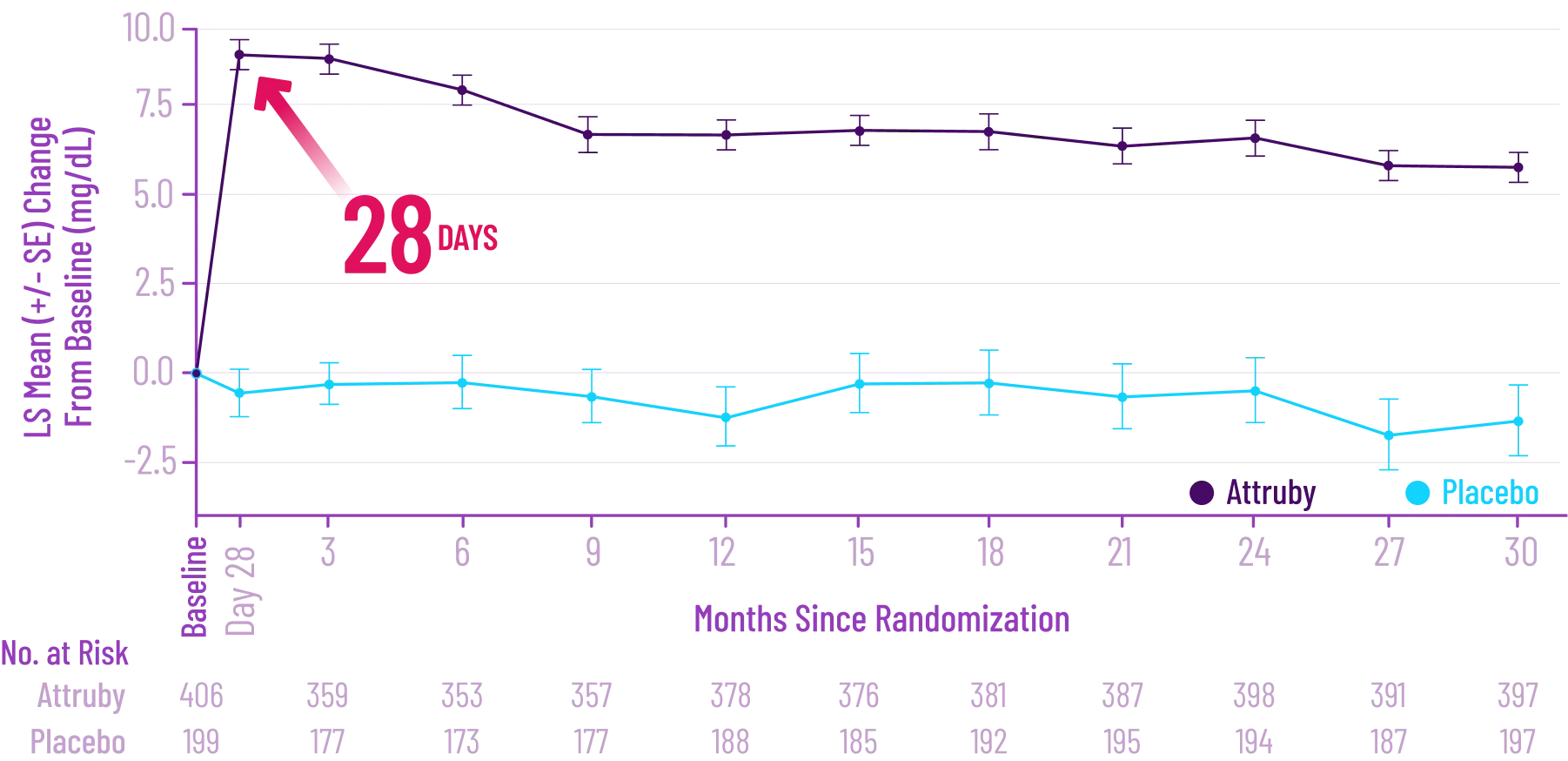
Early increase in serum TTR within 28 days of starting Attruby9
Change From Baseline in Serum TTR Level*
Levels of serum TTR, also known as prealbumin, are a measure of TTR stability13
IN 2 SEPARATE POST HOC EXPLORATORY ANALYSES
Early increases in serum TTR were associated with improved outcomes
Based on logistic model prediction14†
Based on Cox proportional hazards model15‡
Based on Cox proportional hazards model15‡
These exploratory analyses are based on participants from the ATTRibute-CM phase 3 clinical trial for whom serum TTR levels were available at both baseline and Day 28 and may not fully reflect the broader patient population. Additionally, this effect may not be generalizable to other TTR stabilizers.
*Per standard protocol, any missing values were imputed as placebo values.16
†Independent study in 557 patients with ATTR-CM from the ATTRibute-CM study. Univariate analyses in both the overall population and the Attruby-treated population; change in serum TTR remained an independent predictor of ACM even after adjusting for baseline demographic variables, diuretic use, NYHA class, baseline serum TTR, TTR variant or wild-type status, and National Amyloidosis Centre stage.14
‡Analysis of the mITT population of ATTRibute-CM. Combined outcomes of serum TTR CFB to Day 28 and Month 30, and first CVH or cardiovascular mortality, excluding those events that occurred prior to Day 28. Patient stratification was based on treatment group, baseline TTR (<20 or ≥20 mg/dL), and original randomization factors of TTR genotype (wild-type vs variant), NT-proBNP (≤3000 or >3000 pg/mL), and eGFR (<45 or ≥45 mL/min/1.73 m2).15
ACM=all-cause mortality; CFB=change from baseline; CVH=cardiovascular-related hospitalization; CVM=cardiovascular-related mortality; eGFR=estimated glomerular filtration rate; LS mean=least-squares mean; mITT=modified intent-to-treat; NT-proBNP=N-terminal pro–B-type natriuretic peptide; NYHA=New York Heart Association; RR=risk reduction; TTR=transthyretin.
Indication and Important safety information
INDICATION
Attruby® (acoramidis) is indicated for the treatment of the
cardiomyopathy of wild-type or variant transthyretin-mediated
amyloidosis (ATTR-CM) in adults to reduce cardiovascular
death and cardiovascular-related hospitalization.
IMPORTANT SAFETY INFORMATION
Adverse Reactions
Diarrhea (11.6% vs 7.6%) and upper abdominal pain (5.5% vs 1.4%) were
reported in patients treated with Attruby versus placebo,
respectively. The majority of these adverse reactions were mild and
resolved without drug discontinuation.
Discontinuation rates due to adverse events were similar between
patients treated with Attruby versus placebo (9.3% and 8.5%,
respectively).
Laboratory Tests
Mean increase in serum creatinine of 0.2 and 0.0 mg/dL and a mean
decrease in eGFR of 8.2 and 0.7 mL/min/1.73 m2 was
observed in the
adults with ATTR-CM treated with Attruby versus placebo,
respectively, at Day 28 and then stabilized. These changes were
reversible after treatment discontinuation.
Use in Specific Populations
Pregnancy & Lactation: There are no
data on the use of Attruby in pregnant women. Animal data have not
shown developmental risk associated with the use of Attruby in
pregnancy. There are no available data on the presence of Attruby in
either human or animal milk or the effects of the drug on the
breastfed infant or maternal milk production.
Attruby® (acoramidis) is indicated for the treatment of the
cardiomyopathy of wild-type or variant transthyretin-mediated
amyloidosis (ATTR-CM) in adults to reduce cardiovascular
death and cardiovascular-related hospitalization.
IMPORTANT SAFETY INFORMATION
Adverse Reactions
Diarrhea (11.6% vs 7.6%) and upper abdominal pain (5.5% vs 1.4%) were
reported in patients treated with Attruby versus placebo,
respectively. The majority of these adverse reactions were mild and
resolved without drug discontinuation.
Discontinuation rates due to adverse events were similar between
patients treated with Attruby versus placebo (9.3% and 8.5%,
respectively).
Laboratory Tests
Mean increase in serum creatinine of 0.2 and 0.0 mg/dL and a mean
decrease in eGFR of 8.2 and 0.7 mL/min/1.73 m2 was
observed in the
adults with ATTR-CM treated with Attruby versus placebo,
respectively, at Day 28 and then stabilized. These changes were
reversible after treatment discontinuation.
Use in Specific Populations
Pregnancy & Lactation: There are no
data on the use of Attruby in pregnant women. Animal data have not
shown developmental risk associated with the use of Attruby in
pregnancy. There are no available data on the presence of Attruby in
either human or animal milk or the effects of
the drug on the breastfed infant or maternal milk production.
You’re about to leave AttrubyHCP.com and visit an external site.
BridgeBio is not responsible for the content or privacy practices of the site you’re about to redirect to.