Reduce combined ACM and CVH frequency.
Keep life in motion.
Attruby significantly reduced the combination of ACM and CVH at Month 301,2
The primary composite endpoint at Month 30 vs placebo included:
All-cause
mortality
Cumulative frequency of CV-related hospitalizations
stratified F-S test

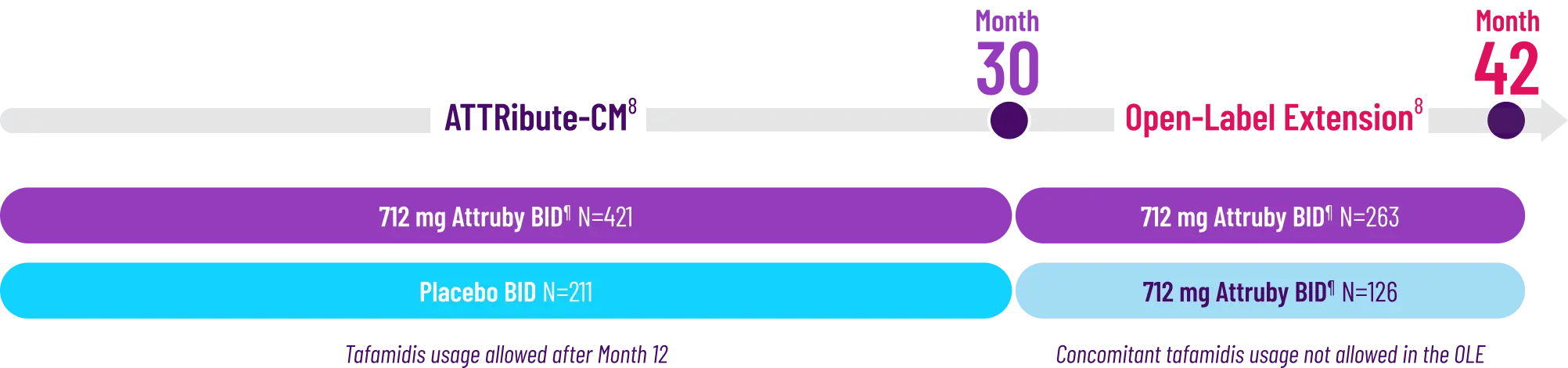
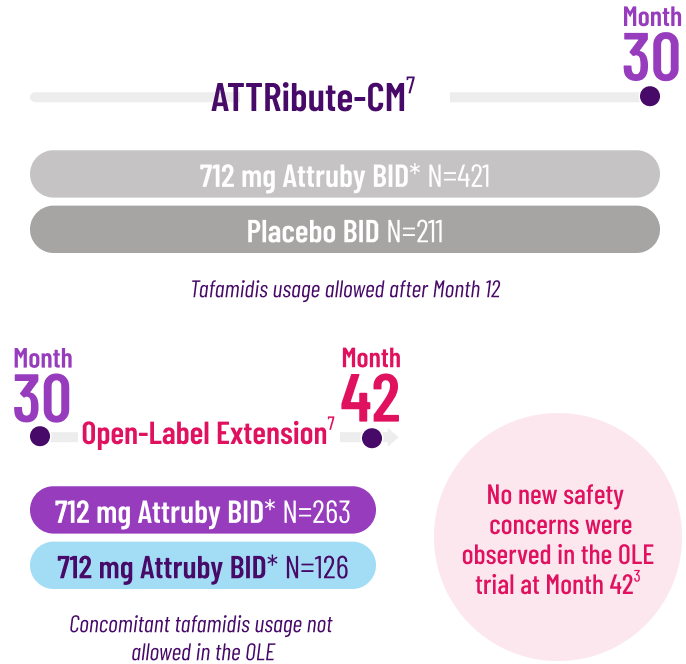
Study Design
OLE Results up to
42 months3
Learn more about the ATTRibute-CM
clinical trial
and the
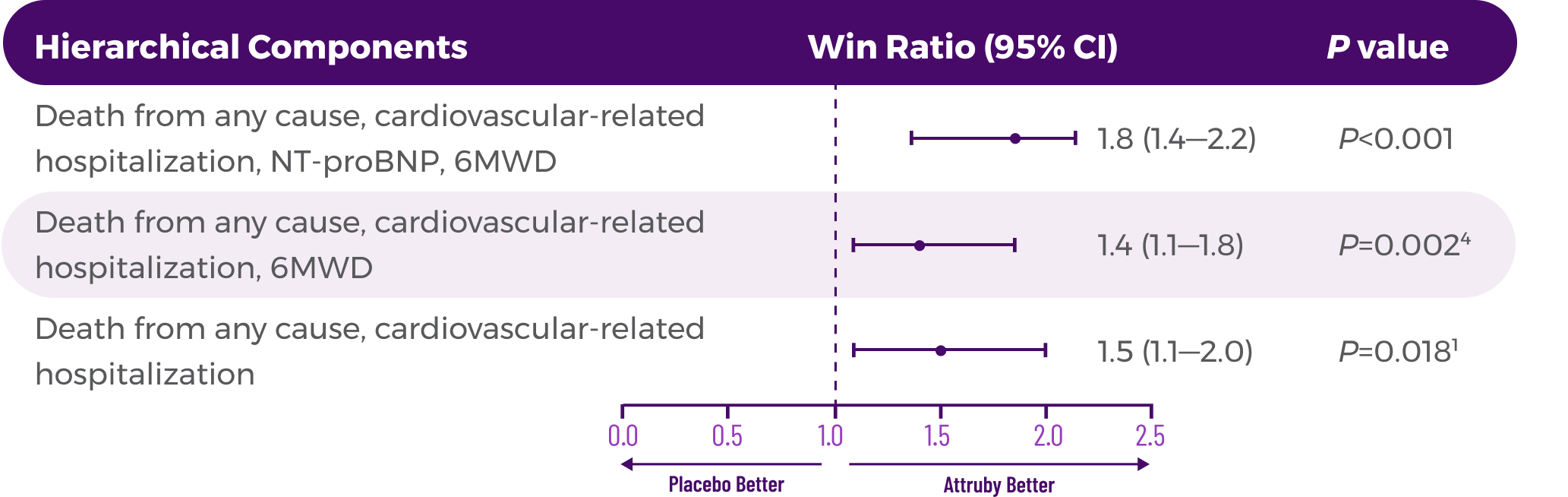
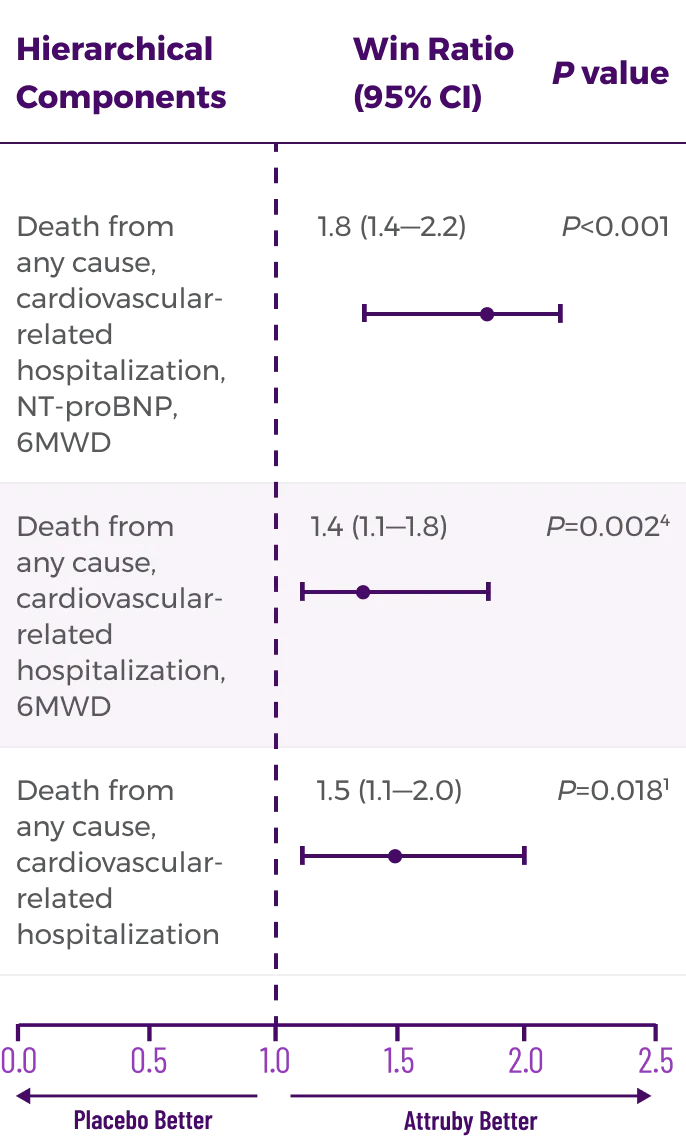
primary hierarchical
composite endpoint
.
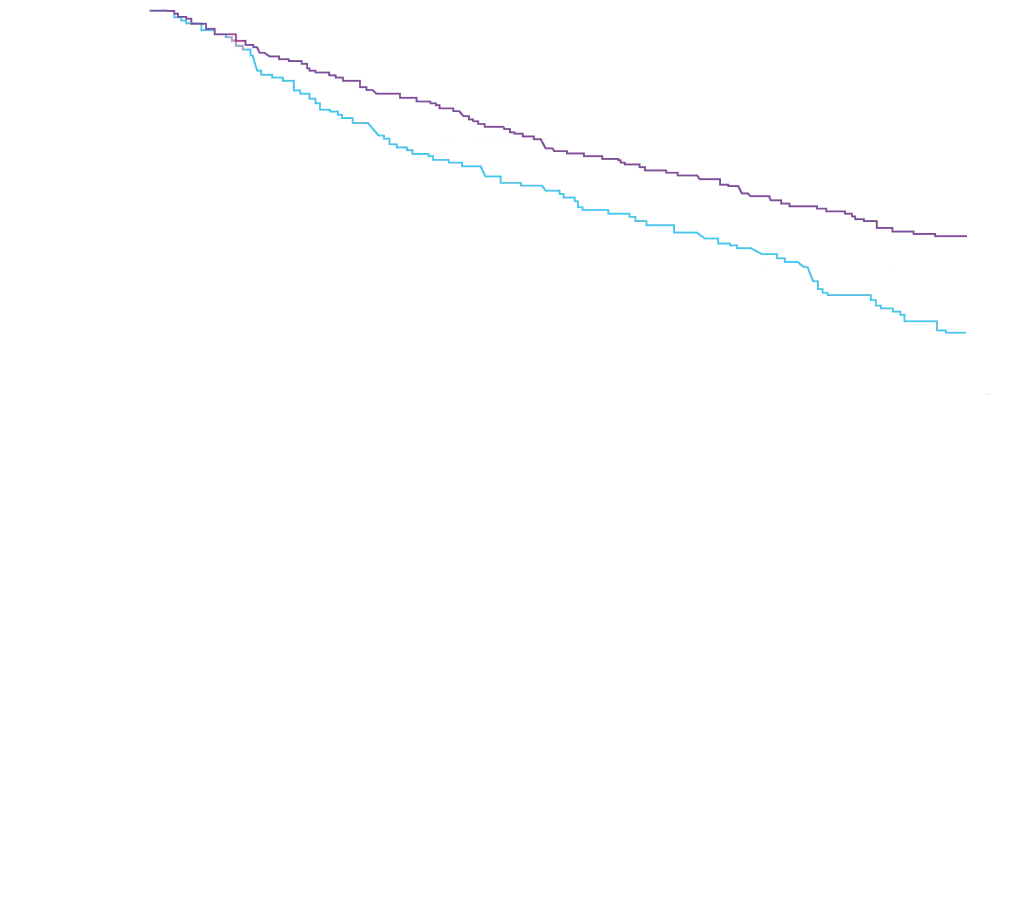
It's not just the impact. It's when you see it.
Attruby showed an early observable difference starting at Month 3
that diverged through 30 months1


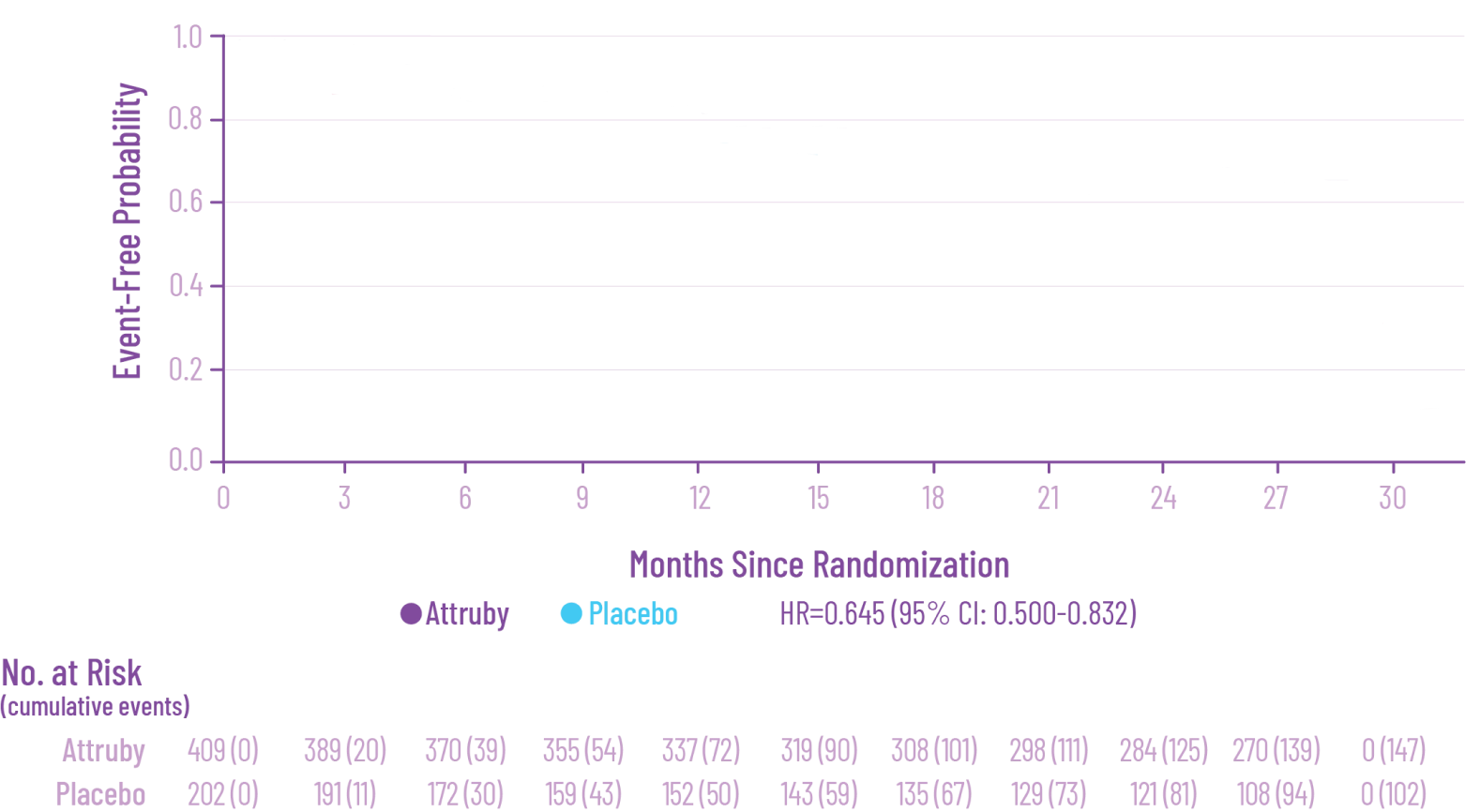

Number needed to treat to
avoid a
death or first CVH
over 2.5 years1: 7
AND RECURRENT CVH4†
THROUGH 30 MONTHS
See results across patients with
wild-type and variant ATTR-CM

 Actor portrayals.
Actor portrayals.
†RRR was calculated using the negative binomial regression model. The total number of
events for Attruby compared with placebo (2:1 randomized) was
79 vs 52 for ACM,
respectively, and 182 vs 170 for CVH, respectively.4
6MWD=6-minute walk distance; ACM=all-cause mortality; ATTR-CM=transthyretin amyloid cardiomyopathy; ATTRv=variant transthyretin-mediated amyloidosis;
ATTRwt=wild-type transthyretin-mediated amyloidosis; CFB=change from baseline; CV=cardiovascular; CVH=cardiovascular-related hospitalization; F-S
test=Finkelstein-Schoenfeld test; HR=hazard ratio; NT-proBNP=N-terminal pro–B-type natriuretic peptide; OLE=open-label extension;
RRR=relative risk reduction.
References: 1. Attruby. Prescribing information. BridgeBio Pharma, Inc.; 2024. 2. Gillmore JD, Judge DP, Cappelli F, et al. Efficacy and safety of acoramidis in transthyretin amyloid cardiomyopathy. N Engl J Med. 2024;390(2):132-142. doi:10.1056/NEJMoa2305434 3. Judge DP, Gillmore JD, Alexander KM, et al. Long-term efficacy and safety of acoramidis in ATTR-CM: initial report from the open-label extension of the ATTRibute-CM trial. Circulation. 2025;151(9):601-611. doi:10.1161/ CIRCULATIONAHA.124.072771 4. Judge DP, Alexander KM, Cappelli F, et al. Efficacy of acoramidis on all-cause mortality and cardiovascular hospitalization in transthyretin amyloid cardiomyopathy. J Am Coll Cardiol. 2025;85(10):1003-1014. doi:10.1016/j.jacc.2024.11.042 5. Gillmore JD, Judge DP, Cappelli F, et al. Efficacy and safety of acoramidis in transthyretin amyloid cardiomyopathy [study protocol]. N Engl J Med. 2024;390(2):132-142. doi:10.1056/NEJMoa2305434 6. Alexander KM, Davis MK, Akinboboye O, et al. Efficacy of acoramidis in wild-type and variant transthyretin amyloid cardiomyopathy: results from ATTRibute-CM and Its open-label extension. JAMA Cardiol. Published online November 8, 2025. doi:10.1001/jamacardio.2025.4477 7. Judge DP, Gillmore JD, Alexander KM, et al. Long- term efficacy and safety of acoramidis in ATTR-CM: initial report from the open-label extension of the ATTRibute-CM trial. Circulation. 2025;151(9) (suppl 1):1-4. doi:10.1161/CIRCULATIONAHA.124.072771 8. Data on file. BridgeBio Pharma, Inc.; 2024-2025.